
If you have had to use a breast pump, you have also had to clean its parts. If you cleaned the parts, you probably did so after each pumping session, which is what the Centers for Disease Control (CDC), and many evidence-based websites recommend. Cleaning requires, at a minimum, rinsing with soap and water, though most advice givers, including the CDC, say to put the parts in a basin of soap and water. The same advice and logic holds for cleaning bottles. The logic behind both sets of advice is that bacteria can grow on any surface, especially one with organic compounds such as milk, and these bacteria could be bad for the child, so they should be removed as much as possible. A couple that is not able to exclusively nurse (for instance, exclusively pumping or combo feeding or needing to pump at work) is therefore compelled by a homogenous wall of advice to religiously clean after each feeding session.
While this advice has a reasonable logic to it, what no one talks about is the cost of the cleaning. Based on my wife’s experience, each cleaning session takes about 5’. The cleaning is especially onerous during late night pump sessions. 5’ is not long in itself, but it adds up over the course of a day. In addition, one is supposed to sanitize once per day. Since new parents are acutely sleep deprived, any time not spent feeding, calming, or sleeping is time wasted, leading me to wonder: just how bad would it be to not clean breast pump material?
When reading about bottle hygiene, it is important to keep in mind the difference between cleaning and sterilizing. Cleaning refers to methods such as rinsing, scrubbing, or wiping, with or without soap, to remove contaminants from an object, in this case a baby’s bottle. While the goal of cleaning is to sterilize, to remove detectable amounts of bacteria, the term sterilization refers to more cleaning that actually does that. Common examples are submerging objects in boiling water, steaming them, or using chemical disinfectants.
After a review of the disappointingly small literature, I have decided it is highly unlikely that anything bad would happen to an infant if equipment (pump parts and bottles) are occasionally only rinsed, but cleaning with soap and water is clearly better than just rinsing. Sanitizing produces the cleanest results, but soap and water removes enough bacteria to make equipment have fewer bacteria than what is considered dangerous; it therefore does not make sense to sanitize frequently. I will use soap and water more often than I thought I would before starting this research, but I am not going to worry if equipment is occasionally only rinsed or left in soapy water, especially during night feeds.
I could find no evidence that defines what a clinically safe amount of bacteria is, that is, what amount of bacteria will make one sick and what will not. The threshold for clean is below 10^4 (10,000) colony forming units (CFU) of bacteria per milliliter. I could find no justification for this threshold, which at this point does not surprise me. While it is normal to draw an arbitrary line in a distribution, I could not find a justification for this one. I have no knowledge to doubt it, but it is worth keeping in mind that decisions about safe and unsafe levels of bacteria are in reference to an arbitrary threshold. For example, the authors of the 1991 article “Bacterial Contamination of Human Milk: Container Type and Method of Expression” state that, “Operationally, lower concentrations were assumed to represent normal milk bacterial flora, whereas higher concentrations were assumed to represent potentially pathogenic bacterial contamination.” Yet a 1998 article examining cleaning and sanitation methods against Bacillus cereus references food safety studies to suggest a dangerous range is 10^3-10^5 (1,000-100,000). The point is simply that there does not appear to a definite amount of bacteria that is safe or dangerous. I could find no evidence connecting bacteria concentration to negative clinical outcomes; while it makes sense that more of a bad bacteria is worse than less of a bad bacteria and the dangerous dosage amount probably varies by enfant, it is surprising that Medicine does not have a better way to demarcate “bad” than folk wisdom. Lacking this clarity, it is perhaps not surprising that advice errs towards caution, but caution also must be weighed against its cost.
While there are few studies that help answer this question, there are at least more than for the 8-12 feedings rule. (For example, the 2016 article “Safe management of expressed breast milk: A systematic review” catalogued only six studies looking at the effect of disinfection and cleaning on bacteria in expressed breast milk. Another study from the same year, “Methods of milk expression for lactating women”, found four.) Also unlike that rule, it turns out that the advice is reasonable. Reviewing the academic literature, it is clear that sterilizing, rinsing with soap and water, and rinsing lower bacteria counts, though sterilizing does not appear to be necessary to lower the bacteria under the accepted safe amounts.
One reason there are few studies pertinent to this question is because the majority of the studies focus on neonatal intensive care units (NICU). When infants are born premature, the mom is often asked to use a pump the hospital provides to express milk that is then manually fed to the newborn. It makes sense that those environments place an extreme premium on cleanliness. Neonates have even weaker immune systems than full-term babies, and pumping equipment is shared across moms. Pumps must therefore be as clean as possible; I do not think bottles are used. However, the standards of NICUs should not be the same that parents are held to in their own home when their kids are healthy. Indeed, this lack of relevance motivates the best study I found, a 2019 dissertation titled “Bacterial Composition of Human Milk Pumped and Stored in Real-life Conditions: A Randomized, Controlled Investigation.”
I found two review articles that tickled me. “Methods of milk expression for lactating women” is an exhaustive 2016 review from the Cochrane Database of Systematic Reviews. Of the 41 studies they include, 26 are of mothers with infants in NICU and only 4 look at contamination. They only include 4 because that is how many are “randomized [or] quasi-randomized”, they find no “clinically significant differences” between milk contamination and pump versus manual expression. “Cleaning and sterilisation of infant feeding equipment: a systematic review” is a 2008 study that emphasizes the then-poor (but still not much better) state of knowledge. It analyzes hygiene recommendations from six countries and notes how much they differ, though the difference is primarily around sterilization method. A common finding in those studies produced the best line I read: “Mothers of subsequent babies […] were less likely to follow recommended procedures.” The article reaches the same conclusion I have 14 years later: “The current evidence base provides little information about effectiveness of the range of old and new methods used, and there is no evidence that either manufacturers or health policy makers have identified the problems parents might face in their own homes. Studies are old, of poor quality and largely irrelevant to circumstances in the home in the early 21st century.”
The earliest relevant article I found is by Arthur I. Eidgelman and George Szilagyi, “Patterns of Bacterial Colonization of Human Milk” and was written in 1979. They take bacteria samples from 44 nursing mothers’ nipples and milk. They find mean and median counts of bacteria are above the 10^4 threshold except for Staphylococcus coagulase negative bacteria. The biggest problem with this study is that the samples were analyzed after 2 hours and 12-24 hours of storage for the nipple and milk samples respectively. The results are therefore only relevant when thinking about stored breast milk.
It would take another 20 years for this question to receive attention. “Effectiveness of Cleaning and Disinfection Procedures on the Removal of Enterotoxigenic Bacillus cereus From Infant Feeding Bottles” is a 1998 article that artificially infects bottles with Bacillus cereus, a food borne bacterium that can cause diarrhea, cleans them using 3 methods and sanitizes them with another three. Sanitizing with steam, microwave, or chemicals removes detectable amounts of the bacteria immediately and keeps their levels safe up to 14 hours later. 18 hours after sanitizing, however, bacteria are greater than the 10^4 safe threshold. While these results appear to strongly favor sanitizing, there are two caveats. Interestingly, they find that rinsing with household detergent and warm water and that plus brushing keeps the bacteria well below the 10^4 threshold when performed immediately. If the infected bottles are left alone for 14 hours, only brushing gets the bottle clean enough; by 18 hours, there are 10^5 Bacillus cereus per ml. The below figure shows this result.

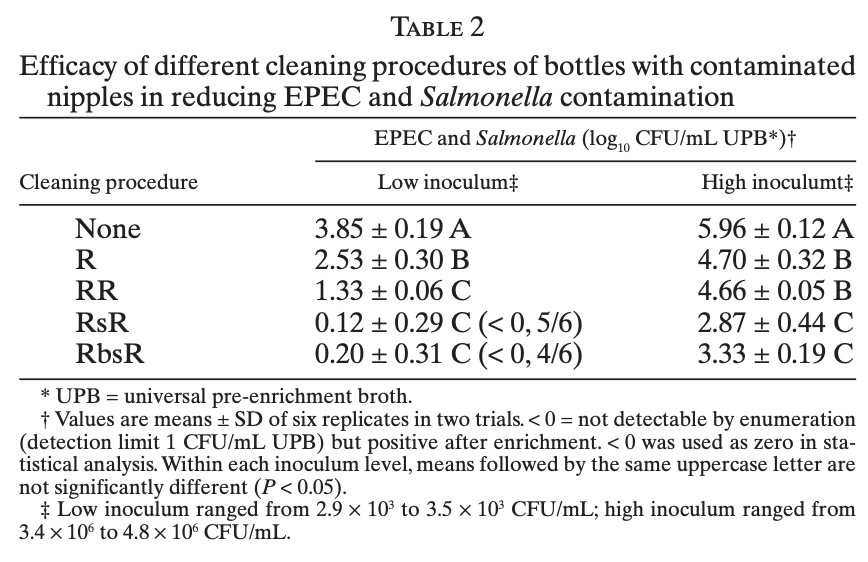
“Efficacy of Protocols for Cleaning and Disinfecting Infant Feeding Bottles in Less Developed Communities” is a 2009 article and the second favorite I found. I like this study because they examine bacteria I have heard of, three strains of E. coli and one of Salmonella; they test several types of cleaning, from none to combinations of rinsing, soap, and brushing; and they very clearly explain the study design. They find that whether or not they infect bottles with 10^3 (1,000) CFU/ml or 10^6 (1,000,000), rinsing, cleaning with soap, and then rinsing kills a sufficient number of bacteria. In fact, rinsing and scrubbing without soap is likely to sufficiently clean, though they do not verify it does so when they also infect bottle nipples. They even show that submerging bottles in tap water for 10 minutes and thoroughly rinsing removes most bacteria. Finally, the study sanitizes using a chlorine solution and finds it is effective.
The below image is of Table 2 from this study. “R” stands for rinse, “s” soap, and “b” brush (scrubbing). The key is to look for the rows where the number before the +- is below 4. Rinsing only can produce clean enough bottles, especially when they are clean to start (low inoculum column).
“Bacterial Composition of Human Milk Pumped and Stored in Real-life Conditions: A Randomized, Controlled Investigation”, a 2019 dissertation by Sarah Michelle Reyes Paredes for Cornell (department unclear), is my favorite study I found. It is my favorite because the cleaning practices are the most realistic of any study and measurement occurs in the subjects’ home. It compares bacteria in breast milk collected with 52 women’s own pumps they clean themselves or sterile ones provided by the study; the research design is good. While the mothers’ pumps are much dirtier than the sterile ones, the author makes the difference seem much larger than it actually is by expressing results in response ratios or relative differences. However, Figure 2 in Chapter 2, shown below, undermines the alarmism: most of the samples collected with mothers’ own supplies contain fewer than 10^4 CFU per milliliter. One shortcoming is that cleaning and storage procedures are not described, so no connection is made between at home behaviors and bacteria prevalence.

To summarize, equipment is cleanest when sterilized, scrubbed with warm soapy water, and rinsed, in that order. However, equipment is almost always below the standard cleanliness threshold of 10^4 CFU/ml with just soapy water and can be with vigorous enough cleaning without soap.
Finally, while sterilization removes bacteria, it introduces microplastic particles. The title of this 2022 Nature Nanotechnology says it all: “Steam disinfection releases micro(nano)plastics from silicone-rubber baby teats as examined by optical photothermal infrared microspectroscopy”. To be fair, this article has many of the same shortcoming as the others I look at: it is not clear if the tens of thousands of cumulative plastic pieces a baby will swallow are a dangerous amount, not enough sterilization methods are tested, and the data come from lab conditions that do not reflect real world conditions. Nonetheless, it is important to remember that no action is cost free: optimizing for removing the item measured (bacteria) increases unmeasured contaminants. Sterilization should still be used, but babies will be fine if it is done rarely.
What would better studies look like? Here are several questions that need to be answered for parents to know with confidence just how clean to be.
- What is the baseline amount of bacteria on bottles before breast milk is extracted? Without knowing the answer to this question, it is unclear how much hygiene degrades when milk is added versus how bad it is initially. This question is especially important because many studies start by infecting bottles with bacteria, but how much to use is unclear without knowing a realistic baseline.
- Does the temperature of the water used to rinse and wash affect cleanliness? This question matters because household water often takes a while to get warm.
- Can one soak equipment in warm soapy water for a long time, like more than an hour, and reach the same cleanliness as more intense but shorter methods like brushing and rinsing? If yes, one could save a lot of labor by not actively cleaning equipment after each session.
- What is the bacteria environment like for bottles that contain formula? They should be cleaner because no pump is involved.
